Find the Right Medical Adhesive
Answer these five basic questions to select the ideal adhesive for your medical application.
Certain epoxies that pass USP Class VI specifications are widely used in the medical industry for manufacturing and repairing endoscopes, surgical instruments, catheters and many other medical devices. Photo courtesy Master Bond Inc.

Medical-grade silicone compounds can be formulated for optical clarity and flexibility to use in potting and encapsulation applications for medical devices. Photo courtesy Master Bond Inc.

One-part, medical-grade, UV-curing adhesives cure fully upon exposure to LED light at a wavelength of 405 nanometers. Certain formulas resist various sterilization methods, yet pass the USP Class VI biocompatibility test and ISO 10993-5 cytotoxicity requirements. Photo courtesy Master Bond Inc.

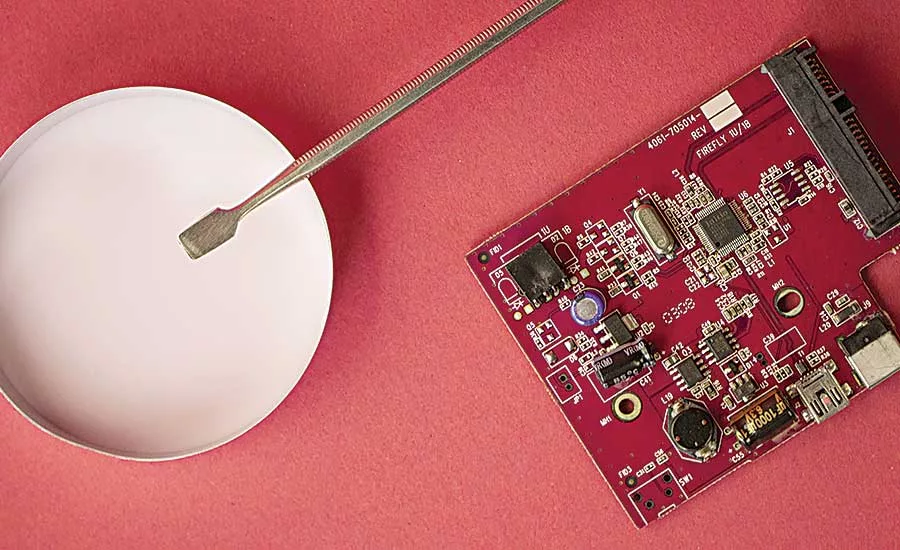
Electrically conductive epoxy adhesives that meet USP Class VI requirements may be used in medical electronic applications that require biocompatibility. Photo courtesy Master Bond Inc.
Picking the right adhesive almost always entails a balancing act as engineers attempt to find products that meet conflicting end-use and manufacturability requirements. Medical device engineers, who also have to contend with a strict regulatory environment, often have the toughest time striking that balance.
Device engineers have to contend with difficult application requirements—such as high bond strength, thermal performance and chemical resistance. On top of these challenges, they have the added burden of picking materials that are biocompatible. And, they often have to pick materials systems that can withstand aggressive sterilization methods.
Not every adhesive can satisfy all of these requirements, and the ones that can, may not be the easiest to work with on the manufacturing floor. In our experience, difficulties can arise in choosing materials and adhesives that not only work together as a system, but also minimize performance and manufacturability trade-offs.
Finding the medical adhesive that can do it all may not be easy, but answering these five questions is a good start.
1. Is the Adhesive Biocompatible?
One common misconception about medical adhesives involves their biocompatibility. Engineers sometimes believe that U.S, Food & Drug Administration (FDA) regulations require that adhesives be tested for biocompatibility before they can be incorporated in a medical device. Yet, the FDA actually considers only the biocompatibility of the finished medical device, not its individual materials. Engineers have the freedom to select and combine materials as they please, as long as the finished device passes muster with the FDA.
In practice, though, sticking with materials known to be biocompatible makes it more likely that the finished device will be biocompatible. So device engineers rightly favor adhesives and other materials that have been “prescreened” by passing industry-standard biocompatibility tests. The most widely accepted test standard is United States Pharmacopeia (USP) Class VI.
Intended to evaluate the suitability of polymeric materials for direct and indirect patient contact, the USP Class VI regimen consists of a series of in vivo reactivity and toxicity tests. These tests involve injecting and implanting samples of the material under consideration into mice and rabbits, which are then evaluated at fixed time intervals for any ill effects.
Looking for quick answers on assembly and manufacturing topics? Try Ask ASM, our new smart AI search tool. Ask ASM
Keep in mind that passing USP Class VI testing doesn’t guarantee that a device will gain FDA approval. All it tells an engineer is that a material has low levels of in vivo toxicity under the test conditions. But, given that a large number of standard adhesives cannot be considered biocompatible, USP Class VI testing represents a valuable tool for identifying products suitable for medical applications.
Master Bond has more than 30 USP Class VI-certified grades of adhesives, not only for bonding but also for related potting, sealing and coating applications. These medical products cover a range of families, including epoxies, UV-curables, silicones, cyanoacrylates, polyurethanes and solvent-based compounds.
2. How Will the Medical Device be Used and Sterilized?
Medical devices that have any chance of patient contact obviously need to be sterilized—either once for disposable devices, like syringes, or even dozens of times for reusable devices, such as surgical instruments. And, the health care industry has an arsenal of methods to make devices sterile, including autoclaving and exposing devices to ethylene oxide (ETO), radiation, electron beams or chemical treatments (for example, Sterrad- and Sterris-type sterilants).
While these sterilization methods do kill microbes, they can also be nearly as tough on polymeric materials. Consider autoclaving, for instance. By far the most popular method for sterilizing reusable devices, autoclaving can subject devices to temperatures up to 135 C and steam pressures up to 20 psi. Many polymeric materials, including a variety of standard adhesives, will start to degrade—primarily through hydrolysis—under repeated exposure to this kind of damp heat. Other sterilization methods tend to be less aggressive than autoclaving, but they each have at least some potential to degrade polymeric materials as the number of sterilization cycles increases.
How the device will be used is what dictates the sterilization method. Disposable devices are typically bulk sterilized a single time as part of their manufacturing process. ETO and gamma radiation have traditionally been the methods of choice, and neither poses a degradation problem for most medical-grade adhesives at that level of exposure.
In disposable-medical-device applications, a wide variety of Class VI epoxies, UV-curables, cyanoacrylates, and silicones adhesives can fit the bill. The choice will depend on the application requirements not related to sterilization.
Reusable devices are a whole different story. The vast majority of these will have to endure multiple trips through an autoclave, possibly even dozens of trips. Or, they may be repeatedly treated with polymer-unfriendly chemical sterilizing agents. For these devices, aggressive sterilization does indeed limit the number of suitable adhesives and polymer substrate materials. Epoxies lead the adhesive pack when it comes to chemical, moisture and thermal resistance. So the majority of autoclave-tolerant adhesives tend to be an epoxy of one kind or another, although other adhesive chemistries can hold up in the autoclave, as well, if the cycles are more limited.
3. How Important is Manufacturability?
This distinction between disposable and reusable devices won’t come as a surprise to experienced device engineers. They know upfront how a device will be used and sterilized, and they design with those constraints in mind. What experienced engineers sometimes do neglect, however, is the relationship between designing for use and designing for assembly. This relationship can be particularly troublesome in medical applications, because the adhesives that offer the best resistance to sterilization aren’t always the fastest or easiest to use on the shop floor.
This trade-off is usually less pronounced with disposable devices. It’s true that disposables—such as syringes—usually have the highest manufacturing volumes, so they truly do need the most productive (easy to use, and fast curing) medical adhesives available. For these applications, there are many Class VI adhesives that require little or no complex mixing, are easy to apply, cure quickly, bond without fixtures and resist common bulk sterilization methods.
Among the popular choices for these high-volume applications are cyanoacrylates, UV-curables and some one-part, heat-curable epoxies. For reusable medical devices on the other hand, it’s just important to keep in mind that a device’s sterilization method can have implications that reach all the way back to the productivity of assembly operations.
While we’re on the subject of productivity, there is an understandable tendency to design as much cure time out of the assembly equation as possible. So all else being equal, engineers will typically favor adhesives that cure at room temperature to avoid the time and expense of a heat cure. In medical applications, where quality and performance are paramount, adhesives formulated to cure at room temperature should still be post-cured with a heat cycle for best results. The reason for the post-cure is to optimize the adhesive’s mechanical and physical properties.
4. What is an Example of a Tough-to-Bond Material That Engineers Need to be Wary of?
One mistake engineers often make is treating the adhesive as an afterthought in the design process. Our technical service engineers have fielded countless calls in which the engineer has picked just the right material to meet their device’s functional requirements—only to find out that they’ve severely constrained their bonding choices.
Given the high level of expertise in the medical design community, this mistake tends to be a nuanced one. It’s not that engineers don’t know that some material families are difficult to bond. (Polyolefins are a classic example.) It’s that they believe there’s always an ideal bonding solution available no matter what substrate materials they choose.
In one sense, they are right. There probably is a solution nowadays for just about every substrate combination, because the adhesive industry continuously makes strides in formulating products that work with tough-to-bond and dissimilar materials. But, the solution may not be “ideal” in the sense that it requires avoidable, expensive trade-offs. To take our classic example, olefinic materials can be adhesively bonded, but they’ll need some help from a primer or surface treatment that adds time and cost to the assembly process.
The point here isn’t to avoid tough-to-bond materials altogether. Sometimes they really are the best choice for the job. Instead, the point is there are many more bonding options available when materials and adhesives are evaluated as a system early in the design process.
5. What’s the Supplier’s Technical Service Phone Number?
The questions we’ve laid out here can help narrow the field when picking a medical adhesive, but they’re really only a start given how quickly the universe of specialized biomedical materials and adhesives is expanding. With each of these new materials comes new questions about biocompatibility, sterilization resistance, bonding performance and ease of assembly. The best way to stay current is to stay in touch with your adhesive supplier.
For further information on Master Bond’s medical-device adhesives, call 201-343-8983 or visit www.masterbond.com.
TYPICAL MEDICAL BONDING APPLICATIONS • Syringes • Sensors • Colostomy devices • Handheld surgical products • Infusion pumps • Lasers • EMI/RFI shielding • Kid-ney dialysis membranes • Catheters • Scopes • Respiratory face masks and systems • Endoscopes • Artificial voice box • Transducers • Prosthetics manufacturing • Lenses • Intra-aortic balloons • Drug delivery devices nd repair • Seals • EGG/EKG equipment • Dental reconstruction • X-ray and imaging equipment • Connectors • Endotracheal tubes • Radio-opaque assemblies • Ven-tricular assist systems • IV kits • Angioplasty devices • Oxygen concentrators • Lap-aroscopic instruments • Hearing aids • Air and liquid filters • Optical electronic devices • Pressure/temperature sensors • Test kits • Diagnostic instruments • Blood heat exchangers • Res-ervoirs • Fiber optics • Suture material systems • Pacemaker components • Valves, pumps and motors • Composites • Artherectomy devices • Prototyping (molding and cast-ing) • Disposable surgical products • Probes • Hip and knee composites. source: Master Bond Inc.
Looking for a reprint of this article?
From high-res PDFs to custom plaques, order your copy today!