Ensuring Adhesion for Medical Device Assembly
There are many factors to consider when adhesives are used to join hard-to-bond plastics.



For medical devices such as catheters, syringes, vials, test tubes and injector pens, many manufacturers are turning to plastics that are formulated to resist harsh chemical and environmental conditions. Growing in popularity are thermoplastic materials, including nylon and nylon derivatives like polyether block amides (PEBAs), as well as cyclic olefin polymers (COP) and copolymers (COC). These materials soften and become pliable on exposure to heat, hardening when cooled to room temperature. They are valued in medical device manufacturing for their strength, their superior mechanical and dynamic properties, and their ability to withstand sterilization and chemicals. They can often replace glass.
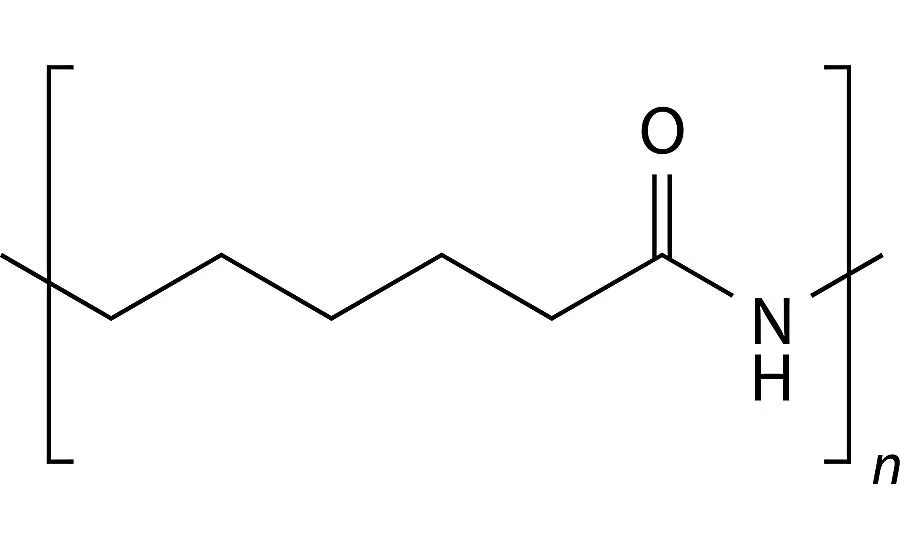
Nylons are semicrystalline polyamide materials that are very tough, offering good thermal, chemical and pressure resistance. These materials deliver the flexibility, tensile strength and compression resistance needed to meet the requirements of devices used for fluid management, surgical procedures and diagnostics. Each type of nylon provides individualized performance characteristics. For example, as the nylon’s associated number increases, specific gravity, melting point and moisture content decrease (nylon 12 has a lower specific gravity than nylon 6).
Extruded tubing made of nylon is lightweight, corrosion and abrasion resistant, and will withstand repeated stress over long periods, making it a popular material for catheter shafts. Nylon is also well-suited for use as a balloon material because of its ability to withstand high pressures in thin-walled sections. Nylon extrusion works well in balloon applications that require more compliance than PET balloons can provide.
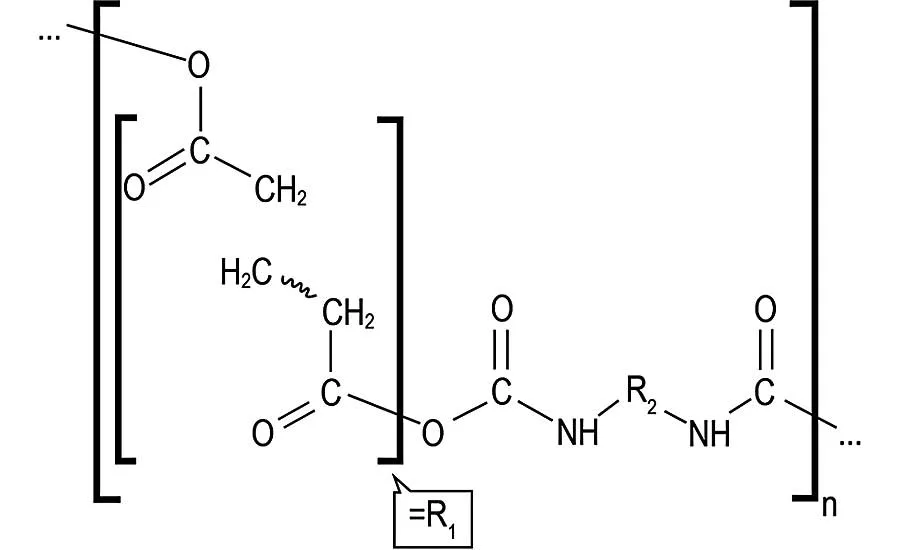
Relatively new to the medical device scene, PEBA is also gaining in popularity. It delivers low friction properties, kink and pressure resistance, softness and flexibility in a chemically resistant, lightweight material. PEBA is a thermoplastic elastomer obtained by polycondensation of a carboxylic acid polyamide with an alcohol termination polyether. Manufacturers are starting to use it in place of common elastomers like polyurethanes, polyesters and silicones because of its lower density, excellent chemical resistance, superior flexibility, and exceptional impact and fatigue resistance. PEBA is gaining popularity for medical films and tubing applications, including catheters and connectors.
COC and COP are relatively new classes of amorphous polymers. Their purity, moisture resistance, clarity and sterilization compatibility make them excellent alternatives to glass in a wide range of medical devices, including syringes and serum vials. Resistant to organic polar solvents, these clear materials allow high light transmission with low haze and chromatic aberration. Absorbing one tenth the water of acrylic (polymethylmethacrylate), they deliver a longer shelf life for liquid contents than other plastic substrates and do not leach at detectable levels. These durable, shatter-resistant plastics will withstand gamma radiation, steam and ethylene oxide (ETO) sterilization.
Assembling Plastic Parts
From fasteners to adhesives, several assembly techniques are available for joining plastic parts. Fasteners such as screws and rivets require a hole—a point of weakness—to be made in the substrate. Therefore, fasteners can only be used on larger, heavier-weight plastic assemblies that will handle the strain and high stress occurring at the insertion site. Ultrasonic welding or fusion bonding involves heating each plastic substrate, then holding the melted edges together and applying pressure until the two parts meld as the plastic cools. This process is effective, but gaps can remain in the assembly due to bond gap variances. In a similar process, solvent welding involves coating plastic parts with a solvent and pressing them together until the solvent evaporates and the parts are fused. This process can result in stress cracking of the plastic substrate.
Plastic parts are most often joined using adhesives, a method that offers distinct advantages over other joining processes. Adhesive bonding is more efficient and easier than alternatives like solvent welding or fastening. Although they require setting and curing time, adhesives easily bond irregularly shaped parts, distribute stress evenly over large areas, bond a wide variety of dissimilar substrates, and seal the bond line. Adhesives create no aesthetic change to the device, since they are applied within the joint and are invisible to the assembly. Light-curable adhesives are especially effective for medical device assembly, because they allow unlimited time for parts adjustment before immediate cure is initiated. Their ability to cure on-demand upon exposure to the appropriate wavelength of light speeds up the assembly process.
Looking for quick answers on assembly and manufacturing topics? Try Ask ASM, our new smart AI search tool. Ask ASM
Plastics fall into two broad categories: thermoplastics, which can be softened and reformed after initial processing, and thermosets, which cannot be melted or reformed. The plastic itself determines the best adhesive for bonding. Certain plastics are considered easy to bond, while others fall into the hard-to-bond category. Especially with plastics, surfaces often need to be prepared to ensure the strongest bond possible.
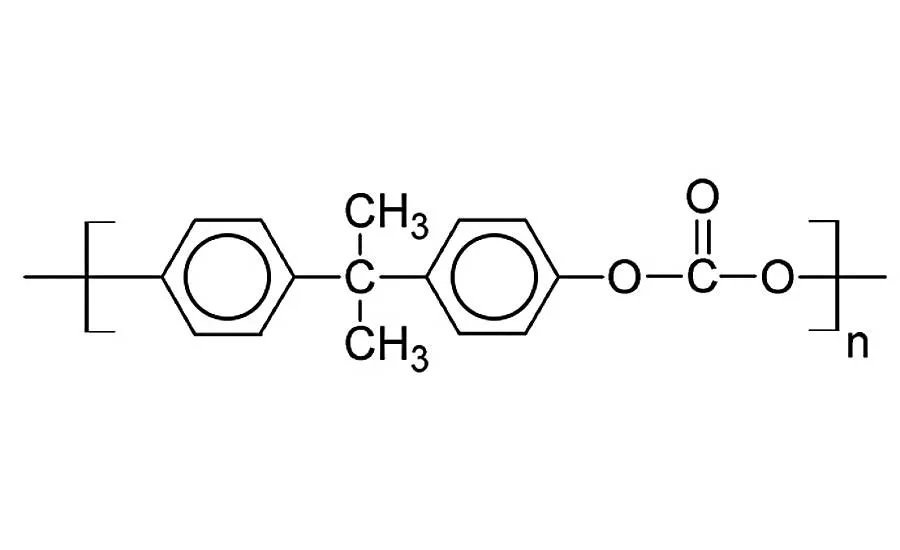
Adhesives want to bond onto reactive groups. Plastics such as polycarbonate and polyetherimide feature carbonyl groups, or carbon atoms double-bonded to oxygen atoms. These plastics are considered easy to bond and are very popular due to the high electron density in the oxygen, which often crosslinks through the double-bond site.
Nylon, COC, COP and PEBA are hard-to-bond thermoplastics. This is due to their low surface energies and smooth, glossy surfaces. Nylon 6 has six nonreactive carbons between bonding sites. Nylon 12 has 12 nonreactive carbons between bonding sites. The greater the distance between bonding sites, the lower the level of adhesion to the thermoplastic. Thus, it’s incrementally harder to bond nylon 12 than it is to bond nylon 6.
PEBAs are a blend of nylon and other resins and are affected by the same bonding issues as nylons. The higher the durometer of a PEBA formulation, the greater the nylon content and the more difficult the material is to bond. When a PEBA formulation’s R2 molecules form a long chain, the chain pushes the bond sites away from each other, increasing bonding difficulty.
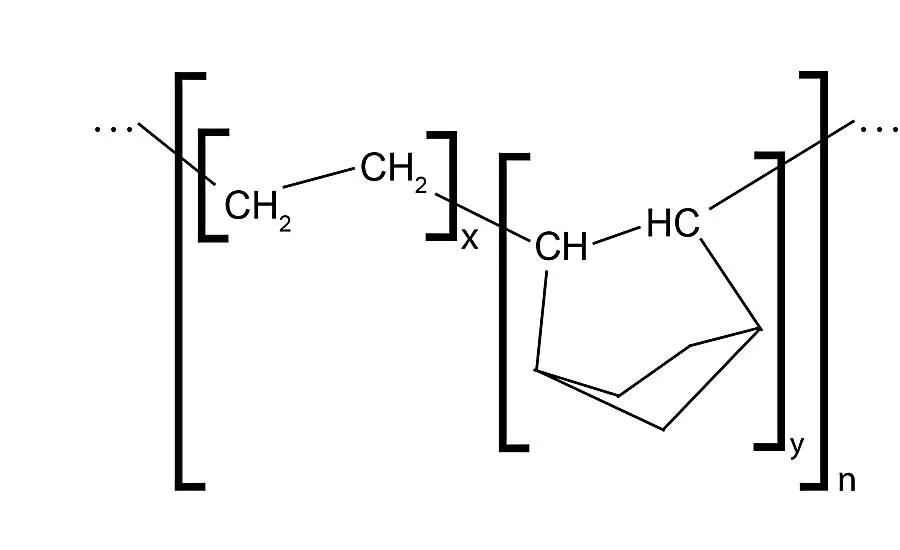
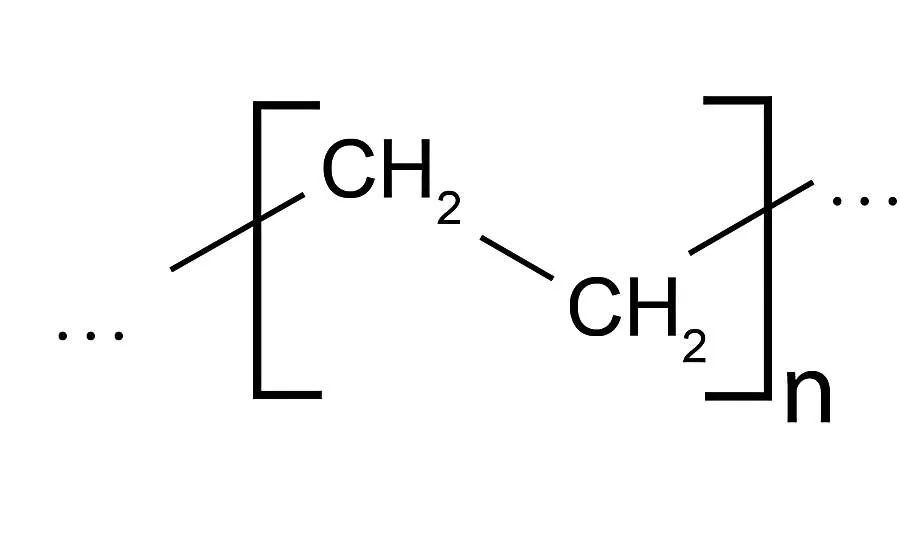
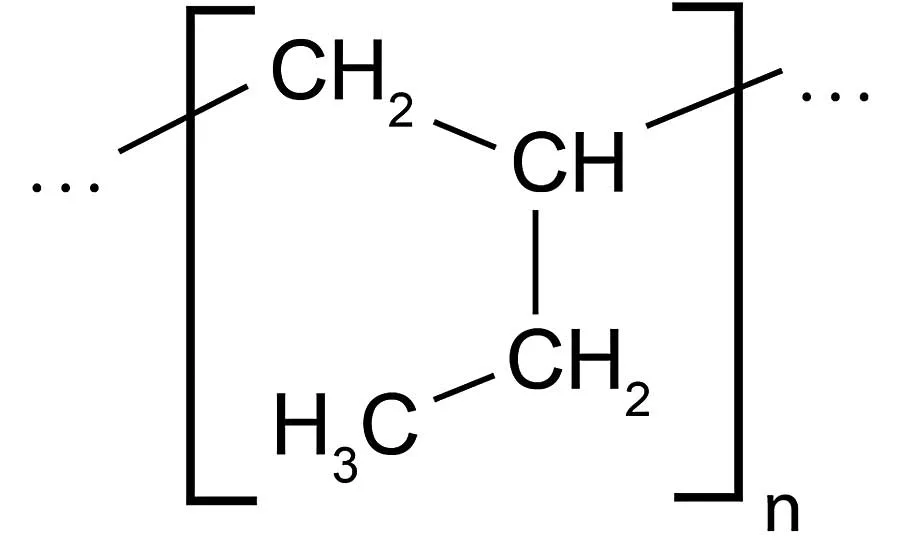
COC and COP are high-clarity copolymers that are difficult to bond because they are composed primarily of ethylene with random interspersed groups of norbornene. Polyethylene (PE) and polypropylene (PP) are also difficult as their chemical formulations provide no natural bonding sites. Soft, flexible silicone has the same bonding problems, since it is very similar in structure to PE. Hard-to-bond plastics usually require some type of pretreatment to obtain good adhesion.
Ensuring a Lasting Bond
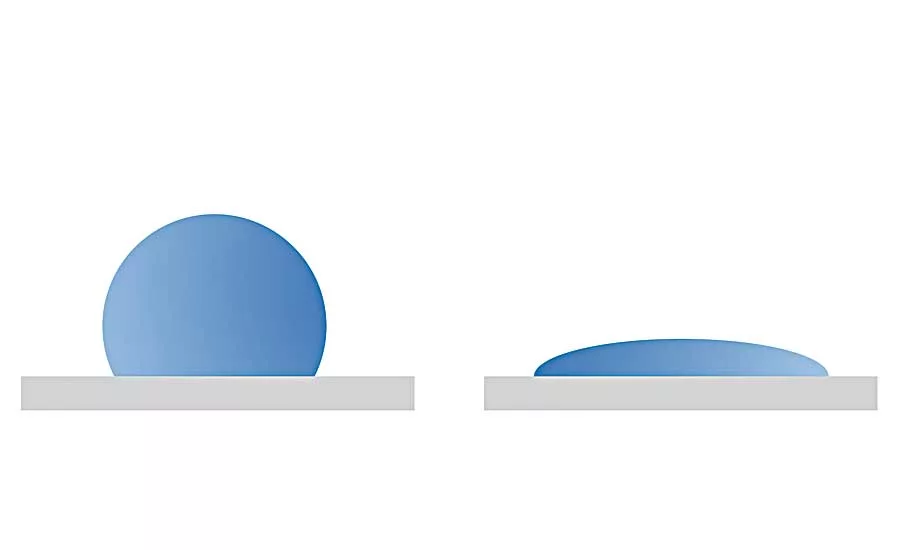
Like plastics, adhesives are polymeric materials with similar physical properties, including surface energies. When a plastic substrate has a higher surface energy than the adhesive, the liquid adhesive “wets” or spreads out in a thin layer over the surface of the plastic. When a plastic substrate has the same or lower surface energy than an adhesive, the liquid adhesive will bead up rather than wet the substrate.
Adhesives that do not wet a surface will not fill surface irregularities, making chemical bonding a challenge. The substrate should ideally have a surface energy that is at least 7 to 10 dynes higher than the adhesive, with most adhesives averaging 34 to 36 dynes per square centimeter. Low surface energy on plastics can also occur for two reasons beyond the properties of the substrate material: surface contamination and low activation of the substrate.
When adhesives do not wet out on a plastic surface, manufacturers can treat the substrate by cleaning the surface to remove contaminants and modifying the surface to improve adhesion. Most surfaces have some level of contamination from dirt, oil, plasticizers, mold release compounds and other
materials. Handling parts can also result in contamination. By cleaning plastic parts prior to assembly, contaminants are removed and adhesion may improve. One of the most common cleaning solvents is isopropyl alcohol.
Several techniques can activate a substrate or change the existing surface to improve adhesion. Grit blasting, micro blasting and sanding will abrade the plastic’s surface and make bonding easier by exposing crystalline microstructures with different wetting characteristics. These abrasion methods physically remove the top layer of the substrate.
Other activation techniques add a surface layer to improve adhesion. Corona discharge is widely used in medical device manufacturing, because it can be done in-line during automated production. During corona treatment, electrons accelerated onto the surface of the plastic create oxygenation, which generates new carbonyl groups with a higher surface energy. This increases reactivity, allowing the adhesive to spread over a larger area rather than bead up. As corona treatment has a limited lifespan, assembly should happen quickly.
Similar to corona discharge, plasma treatment bombards a surface with gases such as argon, oxygen, nitrogen or helium to introduce new amine, acetal, carboxyl or hydroxyl groups to the surface. This increases surface energy, which results in higher bond strength and better wet out.
Chemical treatments involve the application of strong oxidative agents, such as chromic acid, to etch the substrate surface and create a stronger bond. Depending on the plastic formulation, surface wetting can dramatically improve.
Flame treatments will also change surface characteristics. In this process, the plastic passes rapidly through a natural gas flame, the surface melts and a reactive layer of oxidation deposits onto the substrate surface to improve adhesion.
Why do Bonds Fail?
Plastic parts bonded with adhesives can fail over time for several reasons. Plasticizers and stabilizers may be present in the plastic formulation. These chemicals can leach from the plastic during use, weakening the bond. For example, PEBA may be formulated with waxy fillers as stabilizers. These stabilizers tend to migrate to the surface over time, often becoming visible after accelerated aging testing. At high concentrations, these fillers may interfere with bonding or degrade the bonding process, causing adhesives to fail over time.
During plastic manufacturing, mold release agents act as a critical barrier between the mold surface and the plastic, facilitating separation of the cured part from the mold. These release agents can later contaminate the surface of cured parts, affecting adhesive bonding. More effective for molders than polymeric or long-chain agents, monomeric or short-chain release agents are more likely to migrate to the plastic surface and cause bond failure. Monomeric release agents can migrate instantly or over time. The migration process is accelerated by exposure to heat. These agents can chemically attack the adhesive’s link to the surface or physically push the adhesive surface away from the plastic.
Harsh sterilization methods can also induce failure. These sterilization methods, or any high heat and humidity situation, can cause plasticizers like DEHP and BOP to migrate over time from high-concentration areas to low-concentration areas, eventually migrating into the adhesive. This migration causes the adhesive to change color and become gummy or tacky, and can lead to bond failure. To fix the problem, manufacturers can try similar plastic substrates with less mobile plasticizers, or different plastic materials that provide similar
physical properties without the use of plasticizers.
Some plastics degrade because of photo-oxidation on exposure to ultraviolet light. Processors may add pigments like carbon black and UV stabilizers like hydroxyl benzophenone to inhibit the rate of photo-oxidation, but at a cost to the device manufacturer. Similar to plasticizers, stabilizers will also migrate to the surface over time and degrade the adhesive bond, causing joint failure.
Effect of Sterilization Methods
Medical devices must often be sterilized before use. Many factors can affect a device’s ability to withstand sterilization including the sterilization method itself, the adhesive formulation, substrates, joint designs and—in needle bonding—cannula gauge sizes. Typical sterilization methods include autoclaving, ETO, gamma radiation, electron beam (E-beam) and hydrogen peroxide gas plasma.
Autoclaving alone is too aggressive a procedure for most plastic assemblies bonded with adhesives. This sterilization method involves exposing the device to steam at temperatures of 115 to 134 C for 15 to 30 minutes under pressure. In these circumstances, most devices manufactured with adhesives fail.
ETO sterilization is a chemical process in which concentrated ETO gas, an alkylating agent, disrupts the DNA of microorganisms and prevents them from reproducing. The process takes place over 12 to 24 hours at 40 to 60 C and 45 to 75 percent relative humidity. Many adhesives are compatible with ETO; however, delamination may occur if stabilizers or plasticizers migrate to the surface of the plastic after exposure to elevated temperatures.
Gamma sterilization involves exposing medical devices to penetrating radiation, and is commonly used on syringes, needles, cannulas and IV sets. Gamma is known to affect both plastic substrates and cured adhesives by causing “chain scission,” which results in increased tensile strength and reduced elongation. Gamma sterilization also polymerizes uncured adhesives.
Similar to gamma radiation, E-beam sterilization uses high-energy electrons as a radiation source. Produced by normal electrical current, the electrons are accelerated using a linear accelerator to near the speed of light. The resulting energies penetrate materials and destroy the DNA chains of microorganisms. Because the dosing rate is much higher than that of gamma radiation, less exposure time is required and polymer degradation is reduced. Like ETO and gamma sterilization, E-beam sterilization has no expected negative effect on the adhesive, but repeat exposure can break down the plastic substrate, a situation that can potentially affect the bond joint.
Hydrogen peroxide gas plasma sterilization is a five-stage process that generates free radicals to sterilize a wide range of medical instruments in one to four hours. This low-temperature process may be less damaging than other sterilization techniques, but much is still unknown about its effects on substrates and adhesive bonds. Thorough testing is the best method to determine a device’s ability to withstand exposure to hydrogen peroxide gas plasma.
Accelerated aging tests, which involve exposing the device to elevated temperatures over time, can help manufacturers predict the life of plastic devices with chemicals that can leach as well as those treated with harsh sterilization procedures.
Finding the “Right” Adhesive
A number of adhesives can be used to assemble catheters, syringes and other medical devices to deliver high-strength bonding, sealing, gap filling and easy in-line processing. For low-volume, manual assembly operations, two-part epoxy and cyanoacrylate adhesives will permanently secure components. However, epoxies require hours to set and cure with high levels of work in process. Cyanoacrylates offer virtually no time to reposition parts and tend to experience “blooming,” the formation of a hazy white discoloration on nearby surfaces that can negatively impact aesthetics.
For high-volume, high-speed automated production, UV- and visible light-curable adhesives fully cure in seconds to thermoset polymers that form lasting bonds to a variety of plastics, including difficult-to-bond plastics. These one-part adhesives eliminate work in process by curing rapidly on exposure to the right intensity and wavelength of light. They can be formulated with fluorescing properties to allow for easy bond-line inspections to detect adhesive coverage and volume. Some adhesives offer color-change technology that allows manufacturers to confirm cure.
Light-cure adhesive formulations are available from thin-wicking (Newtonian) grades to thixotropic gels that flow only when agitated or stressed. Cure can take as little as 1 to 30 seconds, depending upon the color of the substrate, the depth of the joint, and any UV inhibitors present in the plastic. Once cured, these adhesives can achieve a rigid state or remain soft and flexible, depending upon the formulation. They also offer very good thermal and chemical resistance. Bond strength ranges from 100 to 4,000 psi, and failure typically occurs in the substrate before the adhesive joint.
A wide range of light-curable adhesives are available. The correct adhesive for a specific bonding application will be determined based on variables such as the device design and the manufacturing process.
Various viscosities—the ability of an adhesive to flow around parts—are available to suit almost any manufacturing process. Viscosity is measured in centipoise (cP). The higher the viscosity, the thicker the adhesive. Easy-flow Newtonian materials are considered low viscosity. Such a material might have a viscosity of 100 cP. Thicker Newtonian adhesives have viscosities near 5,000 cP, while thixotropic gels approach 20,000 cP. Part geometry, process design, assembly method and speed should be considered to determine appropriate adhesive viscosity.
Light-curable adhesive formulations will accommodate many bond gap thicknesses and have very low risk of blooming or stress cracking. These single-component adhesives are stored at room temperature, have long shelf life, and no pot life. According to industry research, the majority of light-curable adhesives maintain at least 85 percent of their strength after four weeks aging at 60 C.
Substrate color can affect adhesive performance. For example, color can be used to denote cannula size in needle bonding. Manufacturers using light-cure adhesives should know that substrate opacity may vary depending upon the color of the plastic, and should look for colored plastics that are translucent to allow light to penetrate. Certain specialty adhesives are available that are more compatible with colored or less translucent substrates.
Joint Design Considerations
The strength of a device manufactured with adhesives depends upon several factors:
- the properties of the substrates and the adhesive.
- the stresses on the substrates and assembly.
- the amount of surface area in contact between mated parts.
Five stresses commonly affect a joint: tensile, compressive, shear, peel and cleavage. Tensile stress elongates and pulls bonded components apart. Compressive stress squeezes components inward. Shear stresses slide components in opposite directions, pulling them apart lengthwise. Peel stress affects flexible substrates, lifting one substrate back and away from another (like a banana is peeled). Cleavage stress affects rigid substrates and forces the joint to open at one end.
Most adhesives can resist tensile, shear and compressive stresses, but weaken on exposure to cleavage and peel forces. So it’s very important to eliminate cleavage and peel forces from joints during the design process. Careful joint design can eliminate stresses on the bond and joint and will extend and improve the life of an assembly. Successful joint designs deliver the largest possible bond areas and use both mechanical locking and adhesive bonding to secure components.
Parts Inspection
Medical device manufacturers often audit the adhesive dispense process before cure and inspect components after cure to make sure that the correct volume of adhesive has entered the bond line and that full cure has been achieved. These inspection processes can be used to detect missed dispense cycles, undersized and oversized beads of adhesive, air bubbles, and plugged or broken dispense tips.
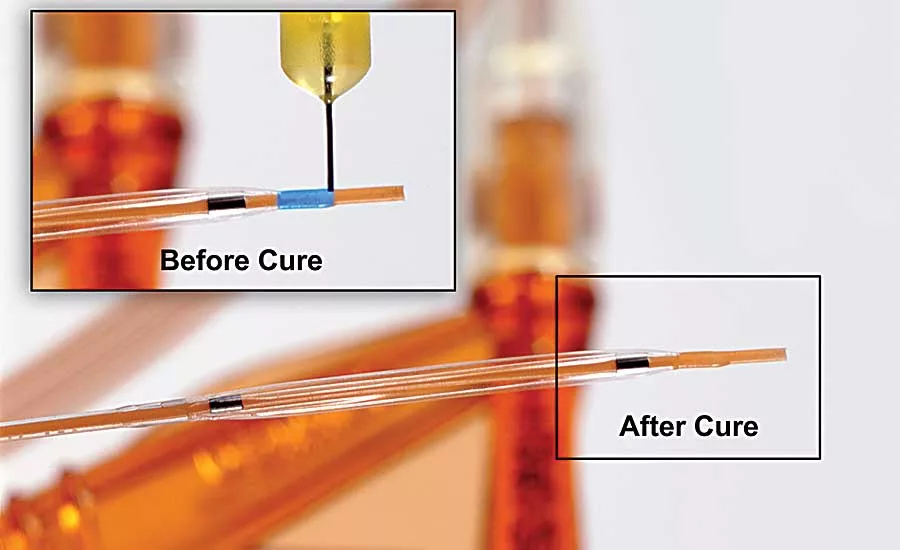
Many light-curable adhesive technologies are formulated to confirm adhesive placement, which can be observed either with the human eye or by vision systems. Some formulations offer color-change technology, in which the adhesive changes from a bright color (e.g. blue) in its uncured state to a lack of color in its cured state. The colored adhesive can easily be viewed to confirm that the correct volume of adhesive has filled gaps after dispensing occurs. By transitioning from blue to colorless, the adhesive allows manufacturers to confirm that cure is complete and the bond has been achieved.
Certain adhesives are formulated with fluorescent dyes that remain colorless until they are exposed to a 365 nanometer black light, at which point they fluoresce red or blue. Adhesives that fluoresce red are particularly effective for use with plastics, such as PVC and PET, that naturally fluoresce blue, allowing easy inspection of bond lines.
Ensuring Reliability
There are many factors to consider when designing with hard-to-bond plastics. Validating the appropriate substrates, adhesive technologies, joint designs, process parameters (including cure equipment), inspection needs, and sterilization techniques are all critical to avoiding failures.
Medical design engineers can narrow their search for the most suitable adhesive by working closely with their adhesive suppliers to thoroughly test prototypes of devices designed with hard-to-bond plastics on simulated assembly lines before actual production has launched. This testing can include dispense and dwell times, cure validation (wavelength selection and cure time), and bond strength evaluations. By conducting research and testing up front, during the design phase, device manufacturers can ensure the success of the assembly during high-volume manufacturing and over the life of the device.
Looking for a reprint of this article?
From high-res PDFs to custom plaques, order your copy today!





