The Ergo Corner: The Tell-Tale Color*
Prevention is the best defense against tendonitis.

 (* In honor of the Jan. 19 birthday of Edgar Allen Poe)
(* In honor of the Jan. 19 birthday of Edgar Allen Poe)
Tendons are one of two main types of connective tissues. (Ligaments are the other.) Tendons can be damaged during heavy or repetitive work. Tendonitis, or inflammation of a tendon, is a common ailment. Tennis elbow and golfer’s elbow are two types of tendonitis; their technical names are lateral epicondylitis and medial epicondylitis.
Once they’re damaged, tendons can be temperamental and finicky. Sometimes they take weeks or months to heal, then quickly succumb to weakness, pain and inflammation upon the slightest provocation. What can account for this exasperating behavior?
The answer is found in the color of tendons.
Tendons are white. The white color is because they have little blood supply. Tendons don’t require a lot of blood because they’re not very active-they just connect your muscles to your bones. That’s why they’re classified as connective tissue. (In case you’re wondering, the average tendon uses 0.1 microliter of oxygen per milligram of dry tendon mass per hour. Now, aren’t you glad you know?)
Muscles are red. The red color is from their vast network of blood vessels. Muscles are very busy fellows, what with all of their contractions, so they need lots of blood to support their active lifestyle. The blood brings oxygen and nutrients and removes waste products from the muscles.
What’s this got to do with tendon repair? The blood supply is the limiting factor in the repair of any injured tissue. Given their good supply of blood, injured muscles usually heal quickly. On the other hand, tendons are limited by their sparse blood supply. Consequently, they heal at a rather pokey pace.
Tendons are amazingly strong. Their tensile strength is greater than that of bone. In fact, fully contracted muscles have been known to break bones. (This is very unusual and is not caused by normal work motions.)
The force on a tendon increases as its muscle contracts. The highest level of tensile stress occurs when the muscle is fully contracted. The bigger the muscle, the greater the stress it can exert on its tendon.
If a tendon is stressed repeatedly and cannot recover quickly enough, the damage starts to accumulate. At first, the damage is microscopic. The collagen fibers of the tendon become damaged, the tendon starts to swell and thicken, which makes the situation worse. A vicious cycle begins. Damage causes swelling, which causes more damage.
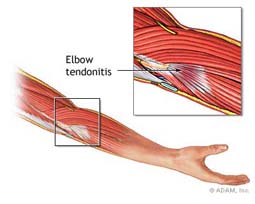
Overexertion injuries in tendons occur most often in the extremities. In the upper body, forceful or repetitive arm motions can lead to tennis elbow and golfer’s elbow. Rotator cuff tendinitis is another common injury and can develop if you work at shoulder level (or higher). In the legs, the most common type of tendinitis affects the Achilles tendon which attaches your calf muscles to your heel bone.
Prevention is the best defense. Tendon problems occur gradually because the damage is usually cumulative. At first, you notice only mild warning signs whenever you use the injured part. Early warning signs are stiffness, weakness or pain. Heed those warning signs. Reduce the strain right away and you may have a reasonably short recovery time.
But if you keep using the injured part, you’ll keep straining it. Damage accumulates until it reaches a critical point. Then the pain can be so bad that you can’t keep working. You’ll have to stop until the tendon heals, which may take months or even years.
Prevent tendon damage by reducing repetition, force, or awkward postures that put a lot of stress on tendons.
Delia Treaster, Ph.D., is a certified professional ergonomist and writes on various ergonomic issues, drawing on decades of experience in occupational ergonomics. She has been an ergonomic contractor with Humantech, one of the largest workplace ergonomics consulting firms in the United States. Prior to working for Humantech, Delia was an ergonomic consultant for the U.S. Postal Service, a senior ergonomic specialist with Travelers Insurance, and a research scientist at Battelle Memorial Institute. She has a master’s degree in human factors engineering and a Ph.D. in biomechanics from Ohio State University.
E-mails to Delia can be sent to ergocorner@yahoo.com.
Editor’s note: “Ergo Corner” is part of a series of guest spots by industry experts that will appear regularly on ASSEMBLY’s blog page. Check back frequently to read more commentaries from Delia, as well as contributions on product testing, automated assembly systems, machine vision and robotics.
Tendons are one of two main types of connective tissues. (Ligaments are the other.) Tendons can be damaged during heavy or repetitive work. Tendonitis, or inflammation of a tendon, is a common ailment. Tennis elbow and golfer’s elbow are two types of tendonitis; their technical names are lateral epicondylitis and medial epicondylitis.
Once they’re damaged, tendons can be temperamental and finicky. Sometimes they take weeks or months to heal, then quickly succumb to weakness, pain and inflammation upon the slightest provocation. What can account for this exasperating behavior?
The answer is found in the color of tendons.
Tendons are white. The white color is because they have little blood supply. Tendons don’t require a lot of blood because they’re not very active-they just connect your muscles to your bones. That’s why they’re classified as connective tissue. (In case you’re wondering, the average tendon uses 0.1 microliter of oxygen per milligram of dry tendon mass per hour. Now, aren’t you glad you know?)
Muscles are red. The red color is from their vast network of blood vessels. Muscles are very busy fellows, what with all of their contractions, so they need lots of blood to support their active lifestyle. The blood brings oxygen and nutrients and removes waste products from the muscles.
What’s this got to do with tendon repair? The blood supply is the limiting factor in the repair of any injured tissue. Given their good supply of blood, injured muscles usually heal quickly. On the other hand, tendons are limited by their sparse blood supply. Consequently, they heal at a rather pokey pace.
Tendons are amazingly strong. Their tensile strength is greater than that of bone. In fact, fully contracted muscles have been known to break bones. (This is very unusual and is not caused by normal work motions.)
The force on a tendon increases as its muscle contracts. The highest level of tensile stress occurs when the muscle is fully contracted. The bigger the muscle, the greater the stress it can exert on its tendon.
If a tendon is stressed repeatedly and cannot recover quickly enough, the damage starts to accumulate. At first, the damage is microscopic. The collagen fibers of the tendon become damaged, the tendon starts to swell and thicken, which makes the situation worse. A vicious cycle begins. Damage causes swelling, which causes more damage.
Overexertion injuries in tendons occur most often in the extremities. In the upper body, forceful or repetitive arm motions can lead to tennis elbow and golfer’s elbow. Rotator cuff tendinitis is another common injury and can develop if you work at shoulder level (or higher). In the legs, the most common type of tendinitis affects the Achilles tendon which attaches your calf muscles to your heel bone.
Prevention is the best defense. Tendon problems occur gradually because the damage is usually cumulative. At first, you notice only mild warning signs whenever you use the injured part. Early warning signs are stiffness, weakness or pain. Heed those warning signs. Reduce the strain right away and you may have a reasonably short recovery time.
But if you keep using the injured part, you’ll keep straining it. Damage accumulates until it reaches a critical point. Then the pain can be so bad that you can’t keep working. You’ll have to stop until the tendon heals, which may take months or even years.
Prevent tendon damage by reducing repetition, force, or awkward postures that put a lot of stress on tendons.
Delia Treaster, Ph.D., is a certified professional ergonomist and writes on various ergonomic issues, drawing on decades of experience in occupational ergonomics. She has been an ergonomic contractor with Humantech, one of the largest workplace ergonomics consulting firms in the United States. Prior to working for Humantech, Delia was an ergonomic consultant for the U.S. Postal Service, a senior ergonomic specialist with Travelers Insurance, and a research scientist at Battelle Memorial Institute. She has a master’s degree in human factors engineering and a Ph.D. in biomechanics from Ohio State University.
E-mails to Delia can be sent to ergocorner@yahoo.com.
Editor’s note: “Ergo Corner” is part of a series of guest spots by industry experts that will appear regularly on ASSEMBLY’s blog page. Check back frequently to read more commentaries from Delia, as well as contributions on product testing, automated assembly systems, machine vision and robotics.